Summary
At Secure Start we offer curricula based on the Triple-A Model of Therapeutic Care and The CARE Curriculum. Both curricula were developed by Colby Pearce, are based in psychological science, but are delivered in an accessible way. Both curricula inform about what you need to know about the therapeutic care of children and young people who have experienced early adversity, and what you need to do to support their recovery and growth.
Each curricula includes complementary training for carers and professionals. It is important that carers and professionals are able to communicate with each other effectively, and having complementary training supports this. Communication supports connection, and supporting therapeutic connections is at the heart of Triple-A and The CARE Curriculum.
Training for professionals incorporates a practice framework that supports fidelity. Professionals are trained in embodying and implementing the model in their practice.
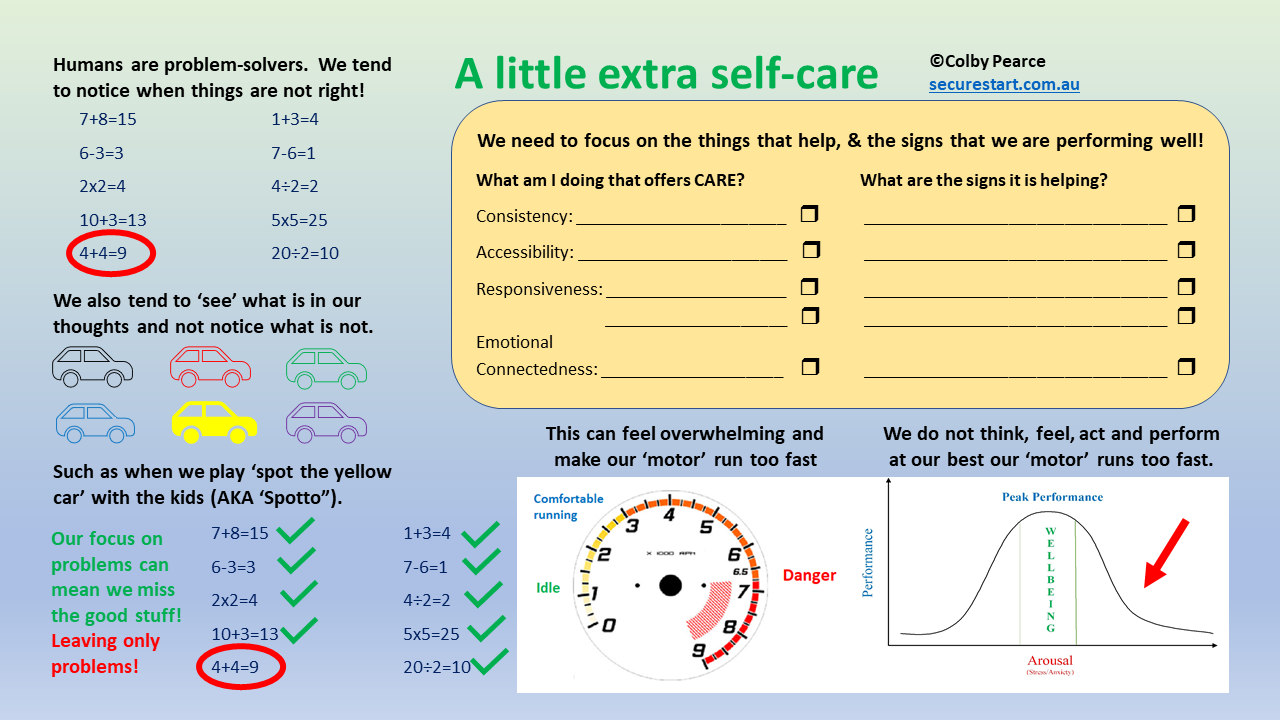
There is a special focus on self-care, in order that participants feel able to realise their aspirations on behalf of children who have had a tough start to life.
Currently, Colby is delivering the Triple-A and CARE Curricula in Australia and Ireland:
- Triple-A is in it’s fourth year of implementation with TUSLA (Child and Family Agency) staff and carers in Donegal, Ireland.
- The CARE Curricula is in its second year of implementation in the Department for Child Protection’s (DCP) Kinship Care Program in South Australia (The Kinship CARE Project).
In 2020 Colby will be delivering training to kinship carers in Victoria, Australia, as part of the Carer KaFE.
For more information, refer below or click one of the related links on the “Training and Curricula” menu tab.
Additional Information
The Triple-A Model of Therapeutic Care and the CARE Curriculum represent evidence-informed conceptual frameworks based in psychological science. Both offer a strengths-based approach that focuses on conventional aspects of caregiving and relating that support optimal developmental outcomes and recovery for children who have experienced early adversity, and the evidence-base for them. The CARE Curriculum is also a practice-framework, whereby it offers a framework for the delivery of accountable support services that promote carer fidelity to the model and optimal outcomes for children.
The Triple-A Model of Therapeutic Care and the CARE Curriculum do not seek to replace other approaches to trauma-informed, therapeutic re-parenting of children, and support for their carers. Rather, the each curricula offers a back-to-basics approach that forms a solid foundation to build on. As strengths-based approaches, the Triple-A Model of Therapeutic Care and the CARE Curriculum complement other strengths-based approaches.
Central to both curricula is the development of knowledge and understanding of the reasons why people behave in the manner that they do and competencies that support these reasons being addressed. This is central to addressing one of the main casualties of grossly-inadequate care – namely, the experience of having one’s needs met reliably and predictably that is the foundation for secure dependency and optimal developmental and interpersonal outcomes. Both curricula endeavour to promote addressing needs as a fundamental caregiving priority, as opposed to simply addressing behaviour(s) of concern in isolation of needs.
The Triple-A Model of Therapeutic Care and the CARE Curriculum promote human Connection as a primary task (Kahn, 2005), where the primary task is defined as the one task that we need to get right and upon which the success of all endeavour rests. There is a robust and ever-growing evidence base for the role of connection in supporting optimal emotional and behavioural outcomes for young people and adults alike (Dooley & Fitzgerald, 2015; Ottman et al, 2006; O’Rourke & Souraya, 2017).
Implementation Projects

The Kinship CARE Project
The Kinship CARE has been implemented successfully with statutory kinship carers in South Australia over the past two years. The Kinship CARE Project is a joint initiative of the Department for Child Protection (DCP) and Secure Start®. At the time of writing, and over the previous 18 months, Kinship CARE Project training has been delivered to 18 groups of kinship carers in 13 metropolitan and 5 regional locations of South Australia. More than 220 kinship carers have attended part or all of the training, with an overall retention rate for attending 4 or 5 sessions (including call-back) of 47%*. This compares favourably with international trends for retention in parenting training (Garvey et al, 2006; Nix et al, 2009).
In the Kinship CARE Project there is a focus on supporting carers to develop an understanding of how to implement a therapeutic re-parenting approach in their own individual circumstances. That is, there is a focus on assisting carers to know what to do, and to develop a tailored therapeutic re-parenting Plan. Psychological theory is presented sparingly and only in support of the rationale (and evidential basis) for recommended approaches. Accessibility of the content is supported through a multi-modal approach to delivery that includes practical activities, demonstrations and audio-visual content in support of verbal content. Regular individual and group reflections also support understanding of the program content. Kinship care support workers regularly attend sessions with carers on their caseload, further supporting caregiver accessibility to the content and shared experience of the Project.
In the Kinship CARE Project there is complementary training for kinship care support workers and psychology staff. The content and delivery is similar to that which is delivered to kinship carers, except that there is a focus on the implementation of the CARE Curriculum in kinship care support workers’ practice with kinship carers, and psychologists’ practice with kinship care support workers. That is, there is a layered approach to implementation, whereby kinship carers experience CARE from their support workers, and support workers experience CARE from psychologists trained in the Curriculum. Implementation is layered in this way to support fidelity to the curriculum and embeddedness across the Department for Child Protection’s Kinship Care Program.
The Triple-A Model of Therapeutic Care
The Triple-A Model of Therapeutic Care was developed for a foster care audience. It was initially implemented as the preferred Model of Care in the Centacare Intensive Family Preservation Foster Care Program in South Australia in 2014/15. Across the past four years the Triple-A Model of Therapeutic Care has been implemented as the preferred Model of Care in the TUSLA (Child and Family Agency) Fostering Service in Donegal, Ireland. In September 2018 twelve local trainers, including 6 members of the TUSLA Fostering Service and 6 local foster carers, were trained as local trainers in the Triple-A Model of Therapeutic Care.
The implementation of the Triple-A
Model of Therapeutic Care in Donegal has been a great success, with successive
reports (2016, 2018) by the independent
statutory inspection authority for health and social care services in Ireland
(HIQA) reporting positively on the Triple-A implementation. A Training Needs
Analysis by the TUSLA Fostering Service in early 2018 reflected that the Triple-A Model of
Therapeutic Care was the most mentioned training when general and relative
foster carers were asked about useful training they had received, including by
a factor of 10:1 over the better-known international approach Therapeutic
Crisis Intervention (TCI).
References
Pearce, C.M. (2010). An Integration of Theory, Science and Reflective Clinical Practice in the Care and Management of Attachment-Disordered Children – A Triple A Approach. Educational and Child Psychology (Special Issue on Attachment), 27 (3): 73-86
Kahn, W. A. (2005). Holding Fast: The Struggle to Create Resilient Caregiving Organisations. Hove and New York: Brunner-Routledge
Dooley, B & Fitzgerald, A (2015). My World Survey: National Study of Youth Mental Health in Ireland. UCD School of Psychology, Headstrong
Ottman, G, Dickson, J, & Wright, P. (2006). Social Connectedness and Health: A Literature Review. Cornell University GLADNET Collection
O’Rourke, H. M., & Sidani, Souraya. (2017). Definition, Determinants, and Outcomes of Social Connectedness for Older Adults: A Scoping Review. Journal of Gerontological Nursing, 439(7), pp 43-52.
Nix, R.L, Bierman, K.L, & McMahon, R.J. (2009). How attendance and quality of participation affect treatment response to parent management training. Journal of Consulting and Clinical Psychology, 77(3): 429-438
Garvey, C, Julion, W, Fogg, L, Kratovil, A & Gross, D. (2006). Measuring participation in a prevention trial with parents of young children. Research in Nursing and Health, 29:212-222
* Nb Data for groups 1-12 only. Final retention data, including for groups 13-18, to be collated at the end of 2019)
Contact Colby
To access a range of free resources suitable for parents/carers, teachers and health/social care professionals, click the image below:
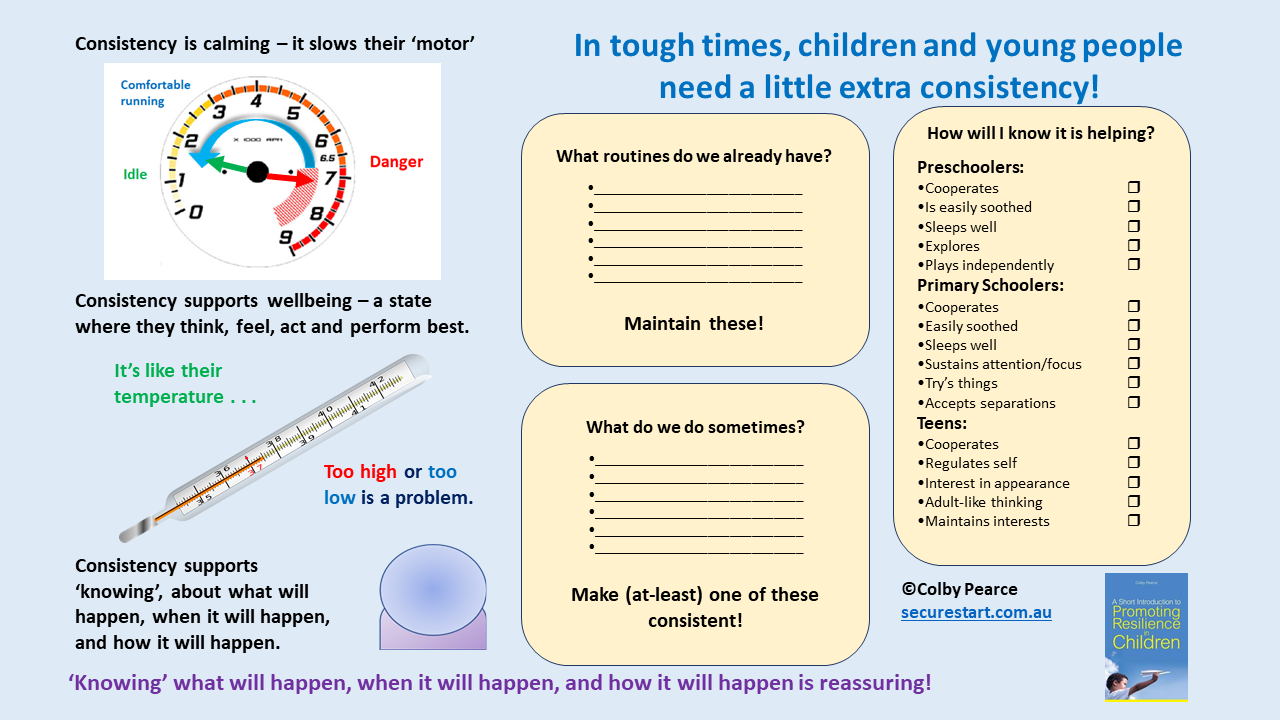
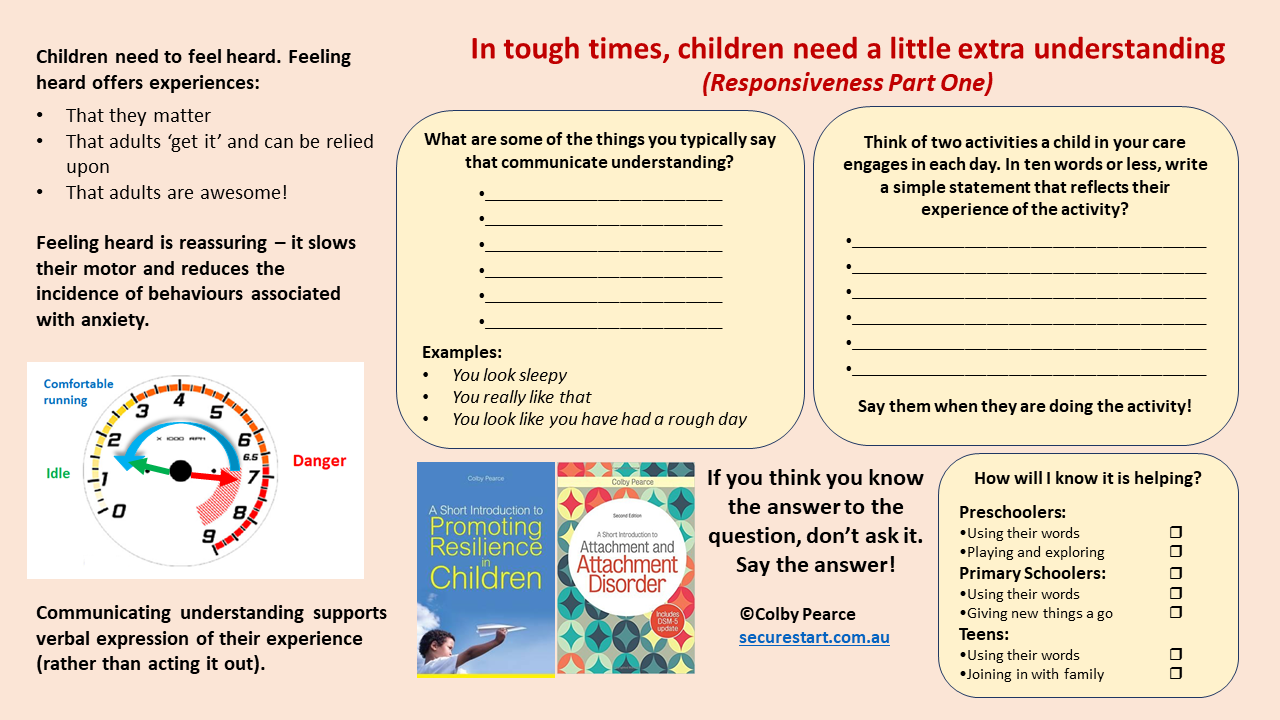
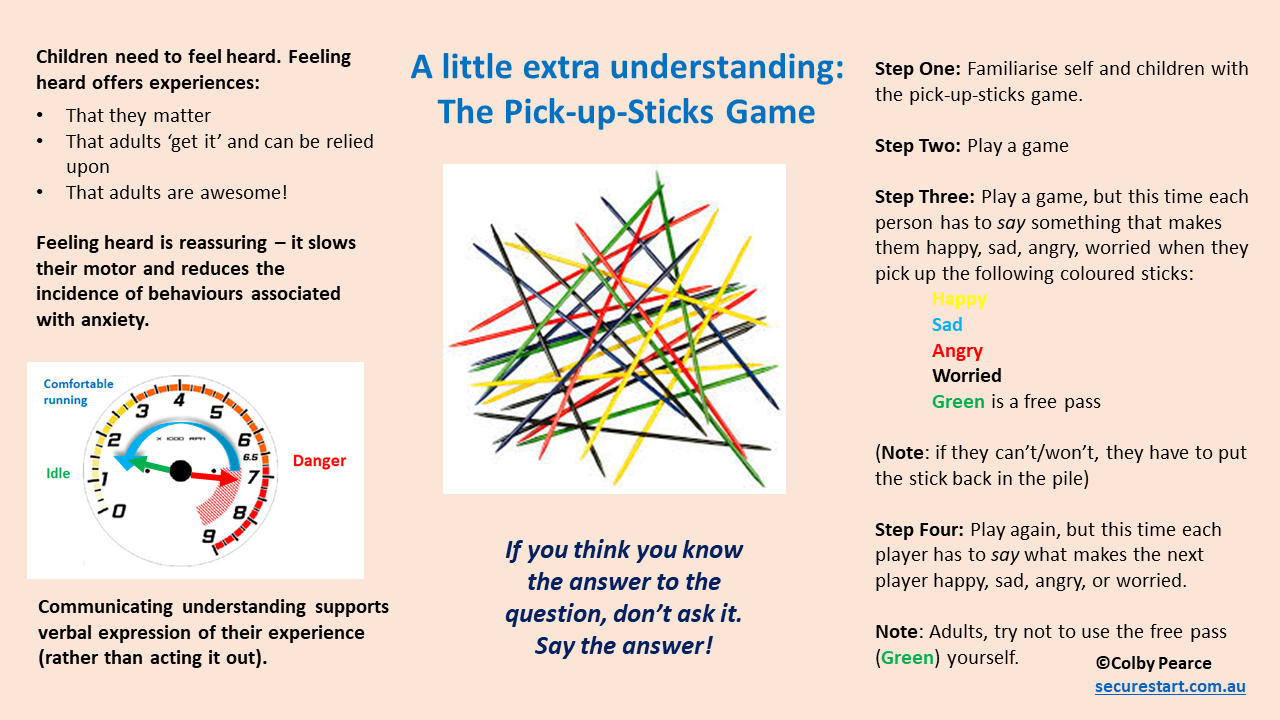
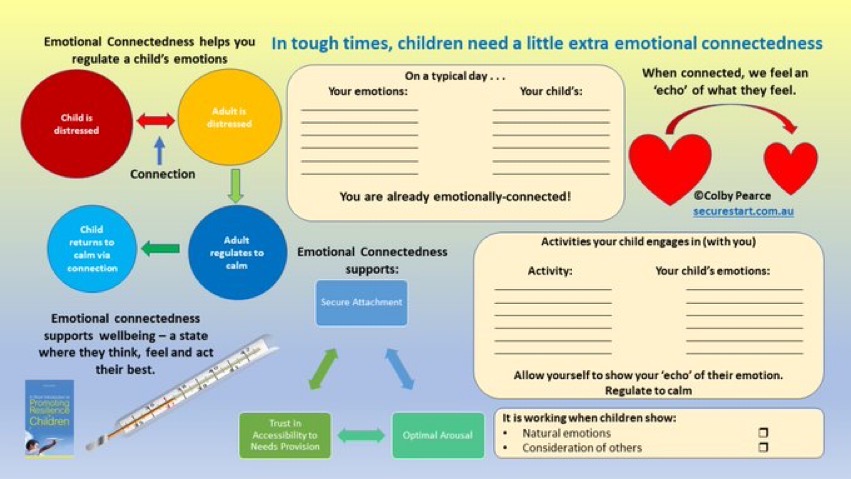
A straightforward guide to keeping things on track in the home during tough times. Includes printable worksheets – see preview below. 18pp
Pay/donate what you want:
Or, download here.
Preview: